

Understanding Prostate Cancer
Atlanta Prostate Center's board-certified urologists deliver specialized care for prostate cancer, including screening, accurate diagnosis, and the full range of treatment options.
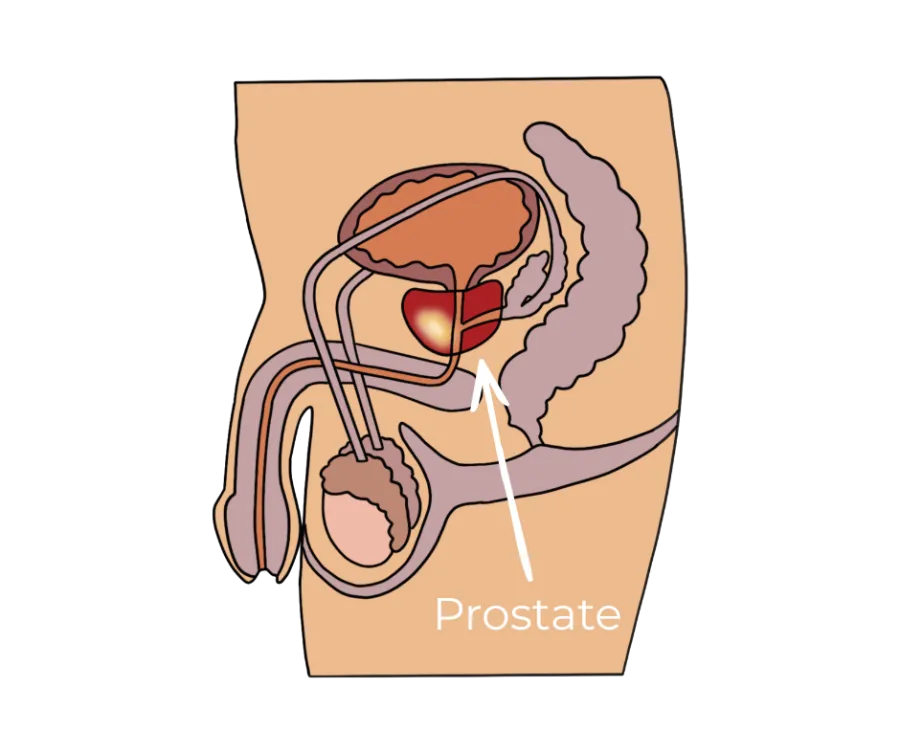
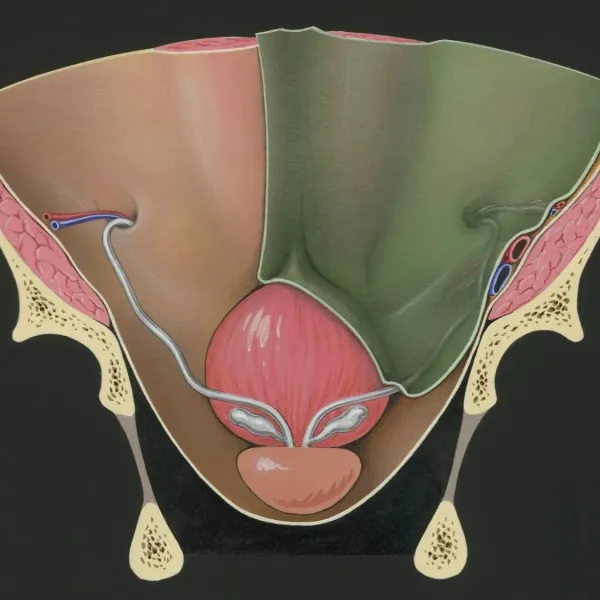
What Is a Prostate?
The prostate is a small gland that sits below the bladder and in front of the rectum. It surrounds the upper part of the urethra, which is the tube urine and semen pass through. The gland's main job is to produce part of the fluid that makes up semen.

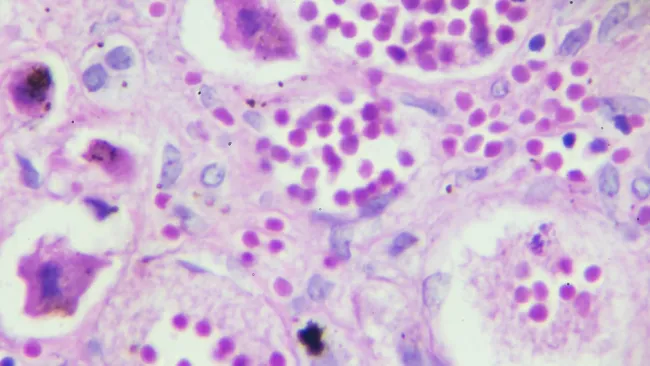
What Is Prostate Cancer?
Prostate cancer happens when cells inside the prostate begin to grow in an uncontrolled way. Many of these cancers grow slowly and stay confined to the gland for years. Others grow more quickly or spread beyond the prostate to nearby tissue, lymph nodes, or bone.
The treatment plan a urologist recommends depends heavily on which kind of behavior the cancer is showing, which is why diagnosis and grading matter so much.
Signs and Symptoms to Pay Attention to
Early prostate cancer often causes no symptoms, which is part of why screening matters. When symptoms do appear, they often overlap with non-cancerous conditions like benign prostatic hyperplasia (BPH) or prostatitis and should be evaluated.
If symptoms come on suddenly or are severe, treat them as urgent and seek care right away.
Changes In Urinary Flow
Trouble starting urination, a weak stream, or interrupted flow
Frequent or Nighttime Urination
Needing to urinate frequently, especially at night
New Erectile Difficulty
Trouble with erections that is new or persistent
Blood in Urine or Semen
Visible blood at any point in either fluid
Lower Back, Hip, or Pelvic Pain
New, unexplained pain that does not resolve
Painful Urination
Pain or burning during urination
Screening: PSA and the Prostate Exam
Most professionals suggest a screening conversation should begin in a man's forties to fifties, depending on personal risk. Two tools are most commonly used for prostate cancer screening:
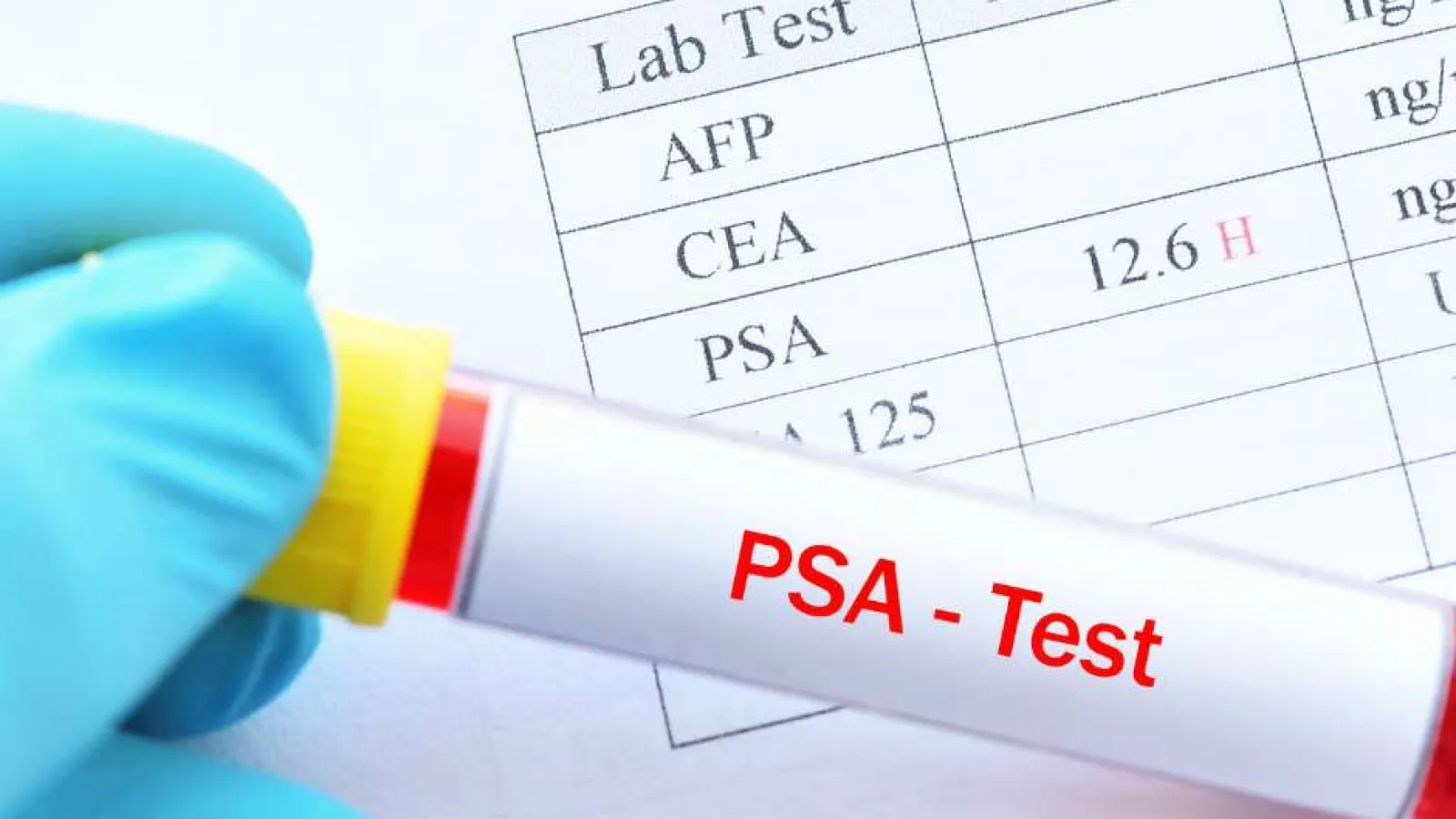
Prostate-Specific Antigen (PSA) Blood Test
PSA is a protein made by the prostate. Levels can rise with cancer, but they can also rise with infection, inflammation, BPH, and even recent activity. A single PSA result is just one piece of the overall picture. Your prior results, age, and prostate size all influence how the number is interpreted.
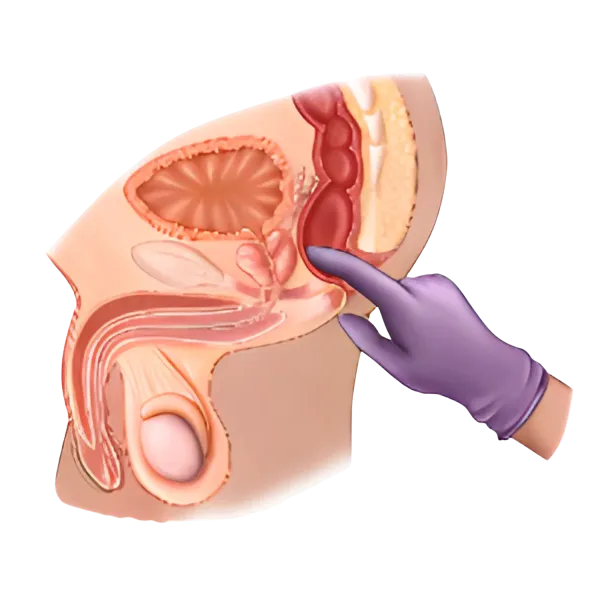
Digital Rectal Exam (DRE)
A brief physical exam that lets a urologist feel the back surface of the prostate for firmness, nodules, or asymmetry. It is not a substitute for PSA, and PSA is not a substitute for the exam; together they give a more complete picture.
How Prostate Cancer Is Diagnosed
If a PSA result, a DRE finding, or a symptom raises concern, a urologist will usually take a stepped approach rather than jumping straight to a biopsy. The goal is to gather enough information to either rule out cancer or characterize it accurately enough to plan the right treatment.


Call Atlanta Prostate Center Today
At Atlanta Prostate Center, prostate cancer care is all we do. If you or a loved one is facing a prostate cancer diagnosis, or you just want a second opinion, we are here to help you find the right path forward.
Treatment Options at a High Level
The right plan depends on the type of cancer, the grade, the stage, your age, and your overall health. Our role is to lay out the choices that fit your situation, explain the trade-offs, and let you decide with us.

Androgen Deprivation Therapy
Prostate cancer cells rely on male hormones, primarily testosterone, to grow. ADT works by lowering hormone levels in the body or blocking them from reaching the cancer. It can be used on its own or paired with other treatments to improve outcomes.
Brachytherapy
Brachytherapy is a minimally invasive form of internal radiation therapy where tiny radioactive seeds are placed directly into the prostate. The radiation targets cancer cells from the inside while limiting exposure to surrounding healthy tissue.

HIFU (High-Intensity Focused Ultrasound)
HIFU uses sound waves to heat and destroy cancerous tissue within the prostate. Because the energy is targeted with extreme accuracy, surrounding healthy tissue is preserved, helping protect urinary and sexual function. HIFU is non-invasive, requires no incisions, and is performed as an outpatient procedure.
Robotic Prostatectomy
Robotic prostatectomy is the surgical removal of the prostate using robotic-assisted technology, giving the surgeon enhanced precision, visualization, and control. The minimally invasive approach means smaller incisions, less blood loss, shorter hospital stays, and a faster recovery compared to traditional surgery.
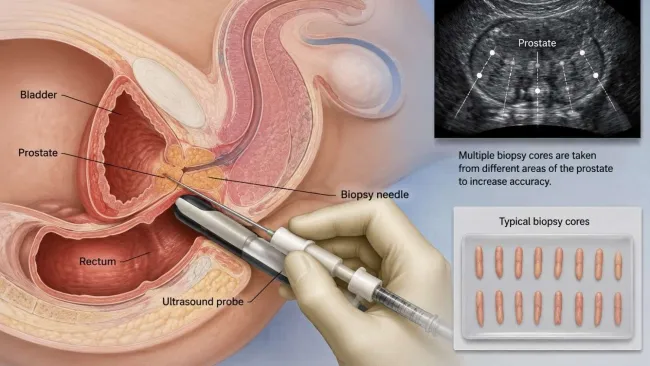
Transperineal Prostate Biopsy
A transperineal biopsy uses MRI and ultrasound guidance to collect tissue samples through the perineum, the area between the scrotum and rectum, rather than through the rectal wall. This approach offers superior accuracy, better access to all regions of the prostate, and a lower risk of infection.

Water Vapor Ablation
Water vapor ablation is a minimally invasive outpatient treatment that uses targeted bursts of steam to destroy unwanted prostate tissue. The thermal energy ablates the targeted area while preserving surrounding healthy tissue and protecting urinary and sexual function.


When to See a Urologist
Prostate cancer often develops without early symptoms, so knowing when to see a urologist matters; consider scheduling a visit if any of the following apply to you.
